
Research Article | DOI: https://doi.org/10.31579/2578-8868/101
Scientific Center BEMCOM, Moscow, Russia.
*Corresponding Author: Alexander Kholmanskiy, Scientific Center BEMCOM, Moscow, Russia.
Citation: Kholmanskiy A. (2019) The geography and demographics of mortality from Alzheimer's disease. J. Neuroscience and Neurological Surgery. 5(2); DOI:10.31579/2578-8868/101
Copyright: © 2019 Alexander Kholmanskiy. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Received: 11 November 2019 | Accepted: 29 November 2019 | Published: 06 December 2019
Keywords: mortality; alzheimer's; education; life expectancy; mentality; level of development
Study nature of epidemiological risk factors and patterns of distribution of mortality from Alzheimer's (MA) in 160 countries. An exponential Malthus model was used to construct adequate approximations of statistical data. Proportionality of average lifetime after 55 years (Δt) to education index (Ψ) was established. Ranking of countries by increasing value of ΨΔt showed that MA depends exponentially on ΨΔt and all countries can be divided into three groups in accordance with level of their economic development. In series of countries of low, medium and highly developed, their average values of MA increase exponentially. Growth of MA in developed countries in post-industrial epoch was explained by emergence of a new risk factor Alzheimer's of a mental nature. A mismatch of complexity or, on contrary, primitiveness of profession with level of mental development of worker, provokes development of chronic stress in him, fraught with pathologies of cognitive function metabolism in elderly. The geography of Alzheimer's disease was explained by the dependence of the human mentality on latitudinal climate change and on the chiral factor of a solar nature acting at night on a sleeping person.
Alzheimer's disease (AD) is the most common form of senile dementia in developed countries [1-3]. AD is considered a multifactorial disease and mutations of certain genes, the mechanism of which is not known, have a leading role in its development [4]. The epidemiological risk factors for the development of AD include age, genetic predisposition, cerebrovascular syndrome, diabetes mellitus [5, 6]. The pathogenesis of AD begins to progress after 55-60 years, when the reproductive component of the hormonal background of brain metabolism weakens, controlled by the epiphysis and pituitary gland. In the same period, defective genes are activated and the protein metabolism of cerebral tissues is disturbed, leading to accumulation of amyloid and tau protein inside cells in the parenchyma and blood vessels of the brain. The deterioration of the rheological parameters of the brain's fluid systems leads to tissue hypoxia and the accumulation of chiral glucose in the blood, which leads to a decrease in the brain's energy potential and the kinetics of metabolic processes. Despite the enormous amount of empirical knowledge about AD, the physicochemical nature and molecular mechanisms of the action of external and internal factors responsible for the etiology and pathogenesis of AD have not yet been established [2]. The absence of these data does not allow to purposefully develop effective and fairly harmless drugs for the prevention and treatment of AD and dementia [3].
It should be noted that the reliability of the patterns of global epidemiology of AD is determined by the adequacy of statistical data on the prevalence and mortality of AD per 100 thousand population (MA) in different countries. Currently, the most accurate are the results of a systematic study of the global regional and national burden of Alzheimer's disease and other dementias for 2016, which takes into account the analysis of the burden of these diseases for 1990-2016 [1]. The scientific inadequacy of statistical data may lead to erroneous results in studies of the nature of the epidemiological risks of AD for a particular region or country. For example, in work [7] it was not possible to establish climatic and ecological justifications for the leadership of Finland in the global MA rating given on the website [8] (Figure 1b). However, according to [1], MA for Finland has a different meaning, which is close to MA for Greece, Spain and significantly less than for Italy and Japan (Figure 1a).
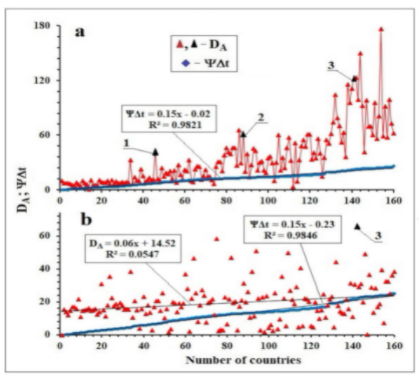
Figure 1: Country rankings and DA values by increasing ΨΔt (Ψ is the education index, Δt is the average lifetime after 55 years). The sequence numbers of countries in the Table. Points (1) and (2) - DA for China and India are not considered rural population, point (3) refers to Finland. Baseline data (a) from [1], (b) from [8].
Thus, the MA analysis carried out in [7] confirms that Finland has no pronounced regional and environmental specificity of the epidemiological risks of AD. The inadequacy of the MA rating in [8] can also be judged by the MA value for Japan, which, it turns out, is an order of magnitude smaller than the MA figured in [1, 9].
Due to the global nature of heliobiology [10] and differences in the energy of sapientation in the countries above and below ~40° nl. [11] when studying the biophysical nature of the epidemiological risks of AD, the role of solar factors must be taken into account. The human body and the brain as a whole is an open water-containing chiral biosystem capable of self-regulation in a narrow temperature range (T = 309-310K) [12]. It is in this range that the anomalous properties of water ensure the stability of homeostasis and effective energy-informational exchange of the brain with the body and with the external environment.

In [11, 12, 13], it was suggested that the specificity of the night period of the circadian rhythm determines the chiral factor (CF) of a solar nature. In part, it is manifested in daily variations in plasma cortisol and melatonin levels [14]. Cortisol affects carbohydrate metabolism, increasing the concentration of glucose in the blood from 4 to 8 hours. Stress intensifies the production of cortisol, increasing the likelihood of diabetes. The maximum content of melatonin in the blood is observed in the middle of a normal night’s sleep at 2-4 am (Figure 2).
It is possible that melatonin can inhibit the formation of amyloid plaques [15, 16]. Violations of the night sleep mode lead to a decrease in the effectiveness of CFSN action and melatonin biosynthesis [17], the deficiency of which can provoke a disorganization of the metabolism at the neurohumoral level [14, 17]. For example, people who systematically work at night increase the probability of the appearance of AD [15, 16, 18, 19], diabetes [20], and also cancer of various organs at women [21, 22] and men [23]. The positive and negative effects of CF and other biophysical factors on the brain or its individual organs can be carried out directly or through sensory systems outside the range of their normal sensitivity. In mice, for example, they found a decrease in the number of amyloid plaques when exposed to sound vibrations at a frequency of 40 Hz [24]. Since this frequency resonates with the γ-rhythm of the brain, it is believed [25] that in a person with AD such a sound can inhibit the formation of amyloids. Such effects are possible due to the acoustic properties of the fluid media of the brain [26] and the resonant connection of its γ-rhythm with the activity of the neurons of the auditory system [27].
Considering the key role of glucose and proteins in the metabolism of a sleeping man’s brain, [12, 14] suggested that their biosynthesis and activity regulates CF and its intensity depends on geography and seasonality.
Thus, it can be considered that hereditary or acquired distortions of the physicochemical bonds of the body with the external environment are the basis of the molecular mechanisms of the etiology and pathogenesis of diseases such as AD, oncology and diabetes. To substantiate this situation, in this paper, we studied the dependences of AD and MA on the characteristics of geography and climate, as well as on the level of education and average life expectancy of the population in 160 countries of the world. To identify the nature of the physical factor regulating the metabolism of the brain in the state of night sleep, we carry out daily and inter-seasonal monitoring of the optical activity of the dextran saline.
Methods and materials
The population loss (ΔN) from AD in different countries for 2016 was taken from [1], and the total population of the countries (No) from [28]. MA per 100,000 population was calculated by the formula: MA = (105ΔN)/No. of the 190 countries in [1] left 160 countries for which there were values of the education index (Ψ) [29] and average life expectancy (tv) in which there were more than 55 years [30, 31]. Symptoms of AD begin to manifest themselves for men and women from ~ 55 years [1]. Taking this into account, we determined the temporal risk factor of AD (Δt, years):
Δt = tv – 55.
Investigated a physiological solution of dextran with a molecular weight of from 30,000 to 40,000 (10 g of dextran and 0.9 g of NaCl per 100 ml of water for injection). The angle of rotation of the polarization plane (o) of light (wavelength 589 nm) was measured on a CM-3 circular polarimeter (measurement accuracy ±0.02o, cuvette 2 dm long). The measurements were carried out at room T (24,5 °C ± 1 °C).
Statistics on mortality from AD in [1] are presented with a 95% uncertainty interval (95% UI). For their processing and graphing used the program Microsoft Office Excel 2010.
Results
The value of Δt is linearly dependent on Ψ (Figure 3a), and a decrease in the statistically average tv value due to MA is insignificant. Considering also the steady increase in tv with the development of countries, ΨΔt can be considered a demographic parameter characterizing the contribution of the population over 55 years old to the country's intellectual potential. The ranking of MA and countries with tv > 55 years, by increasing values of ΨΔt is presented in the Table and illustrated in Figure 1. It contains points 1) and 2) the values of MA for China and India, calculated without taking into account the share of rural (illiterate) population which for these countries amounted to 0.73No [32] and 0.43No, respectively.
The cognitive abilities of a person mainly suffer from AD, which to a certain extent characterizes the value of Ψ, as well as the interval Δt, an increase in which leads to an increase in MA [9]. The population mortality dynamics from AD is subject to the Malthus exponential model and can be formally described by the equation [11]:
MA = (105ΔN)/No = kΨΔt, (1)
here k is a constant (year–1).
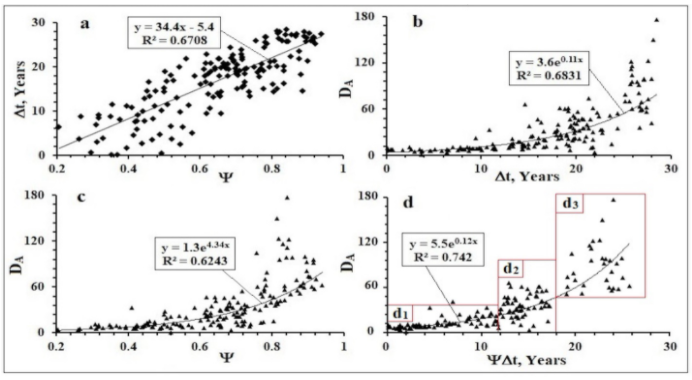
Figure 3: The dependence of the average lifetime after 55 years (Δt) on the education index (Ψ) for different countries (a) and exponential approximations of dependencies of the mortality rate (MA) for different countries on Δt (b), (c) and ΨΔt (d). The rectangles are the countries that are intellectually and economically underdeveloped (d1), moderately developed (d2) and highly developed (d3). Baseline data for countries from [1].
From (1) it follows that MA will be proportional to the exponential exp(kΨΔt). Figure 3 shows that the dependences of MA on Ψ, Δt and ΨΔt are well approximated by the exponents, and the coefficient of confidence of the approximation (R2) has the greatest value with the exponent ΨΔt. The corresponding exponents are applicable for approximations of dependences of the prevalence of AD and MA on the age categories of patients in different countries [1, 4, 9].
№ | Country | ѰΔt | DA | № | Country | ѰΔt | DA | № | Country | ѰΔt, | DA |
1 | Mozambique | 0.04 | 9.67 | 55 | Honduras | 9.4 | 21.5 | 109 | Bosnia Herzeg. | 14.9 | 46.2 |
2 | Guinea-Bissau | 0.1 | 7.04 | 56 | Tajikistan | 9.5 | 7.8 | 110 | Bulgaria | 14.9 | 57.5 |
3 | South Sudan | 0.2 | 7.41 | 57 | Morocco | 9.6 | 27.5 | 111 | Sri Lanka | 15 | 31.9 |
4 | Cameroon | 0.2 | 7.57 | 58 | Egypt | 9.7 | 16.6 | 112 | UAE | 15.1 | 3.4 |
5 | Burundi | 0.7 | 6.32 | 59 | Uzbekistan | 9.9 | 11.6 | 113 | Romania | 15.1 | 51.5 |
6 | Mali | 0.9 | 5.10 | 60 | Suriname | 10.1 | 22.1 | 114 | Bahrain | 15.5 | 9.1 |
7 | Burkina Faso | 1 | 4.79 | 61 | Libya | 10.2 | 20.7 | 115 | Panama | 15.6 | 32.6 |
8 | Equatorial Guinea | 1.1 | 7.61 | 62 | Salvador | 10.5 | 32.6 | 116 | Georgia | 15.8 | 48.4 |
9 | Guinea | 1.3 | 5.91 | 63 | Belize | 10.6 | 10.0 | 117 | Uruguay | 15.9 | 54.9 |
10 | Niger | 1.3 | 4.19 | 64 | Mongolia | 10.6 | 8.7 | 118 | Barbados | 15.9 | 47.7 |
11 | Zimbabwe | 1.4 | 10.23 | 65 | Nicaragua | 10.8 | 22.4 | 119 | Latvia | 16 | 61.0 |
12 | Uganda | 1.6 | 7.26 | 66 | Paraguay | 11 | 26.0 | 120 | Lithuania | 16.1 | 61.2 |
13 | Benin | 1.9 | 5.84 | 67 | Trinidad & Tobago | 11 | 25.2 | 121 | Albania | 16.3 | 33.1 |
14 | Congo | 1.9 | 0.70 | 68 | Kyrgyzstan | 11.2 | 11.3 | 122 | Cuba | 16.4 | 40.9 |
15 | Djibouti | 2.2 | 10.89 | 69 | Azerbaijan | 11.4 | 15.5 | 123 | Slovakia | 16.4 | 41.6 |
16 | Togo | 2.3 | 5.26 | 70 | Dominic. Republic | 11.5 | 22.2 | 124 | Singapore | 16.4 | 34.9 |
17 | Eritrea | 2.3 | 5.53 | 71 | Kazakhstan | 11.6 | 14.7 | 125 | Costa Rica | 16.7 | 56.1 |
18 | Liberia | 2.5 | 5.40 | 72 | Fiji | 11.7 | 14.6 | 126 | Hungary | 16.8 | 39.9 |
19 | Sudan | 2.7 | 10.52 | 73 | Palestine | 11.7 | 10.6 | 127 | Montenegro | 16.9 | 14.8 |
20 | Ethiopia | 2.9 | 8.71 | 74 | Kuwait | 11.9 | 6.3 | 128 | Brunei | 17 | 35.4 |
21 | Zambia | 2.9 | 7.67 | 75 | Colombia | 12 | 25.5 | 129 | Argentina | 17.2 | 54.7 |
22 | Mauritania | 3.1 | 7.83 | 76 | Moldova | 12 | 30.9 | 130 | Chile | 17.2 | 35.8 |
23 | Yemen | 3.1 | 9.81 | 77 | Saint Lucia | 12.1 | 30.6 | 131 | Poland | 19.1 | 50.6 |
24 | Papua New Guinea | 3.2 | 6.87 | 78 | Maldives | 12.2 | 20.5 | 132 | Estonia | 19.1 | 61.3 |
25 | Haiti | 3.3 | 10.76 | 79 | Russia | 12.3 | 37.9 | 133 | USA | 19.2 | 74.1 |
26 | Kenya | 3.4 | 6.78 | 80 | Thailand | 12.4 | 46.4 | 134 | Portugal | 19.6 | 104.3 |
27 | Malawi | 3.5 | 8.96 | 81 | Tunisia | 12.7 | 41.5 | 135 | Cyprus | 19.8 | 79.1 |
28 | Ghana | 3.5 | 7.36 | 82 | Seychelles | 12.8 | 39.4 | 136 | Malta | 20 | 70.0 |
29 | Comoros | 3.9 | 7.19 | 83 | Vietnam | 12.8 | 46.3 | 137 | Czech Republic | 20.7 | 51.9 |
30 | Rwanda | 3.9 | 8.69 | 84 | Ukraine | 12.8 | 46.4 | 138 | Luxembourg | 20.9 | 62.7 |
31 | Senegal | 4.1 | 7.27 | 85 | Samoa | 12.9 | 26.6 | 139 | Greece | 21.5 | 115.9 |
32 | Tanzania | 4.4 | 8.57 | 86 | Slovenia | 12.9 | 65.7 | 140 | Austria | 21.6 | 95.5 |
33 | Pakistan | 4.4 | 8.25 | 87 | Algeria | 13 | 29.4 | 141 | Belgium | 21.7 | 111.5 |
34 | Myanmar | 4.5 | 32.85 | 88 | China | 13.1 | 61.0 | 142 | Finland | 21.9 | 121.6 |
35 | Madagascar | 5 | 6.62 | 89 | Peru | 13.2 | 19.7 | 143 | Spain | 22.6 | 123.0 |
36 | Laos | 5.3 | 14.20 | 90 | Brazil | 13.3 | 39.2 | 144 | France | 22.8 | 98.9 |
37 | Namibia | 5.4 | 9.72 | 91 | Jordan | 13.3 | 14.3 | 145 | Italy | 22.9 | 149.9 |
38 | Solomon Islands | 5.7 | 9.81 | 92 | Grenada | 13.3 | 27.1 | 146 | UK | 23 | 92.3 |
39 | Gabon | 5.8 | 22.58 | 93 | Turkey | 13.6 | 45.5 | 147 | Sweden | 23.3 | 98.2 |
40 | Cambodia | 6.2 | 15.61 | 94 | Belarus | 13.6 | 42.8 | 148 | Denmark | 23.3 | 69.9 |
41 | Botswana | 6.3 | 8.83 | 95 | Venezuela | 13.6 | 21.3 | 149 | South Korea | 23.3 | 69.5 |
42 | Guyana | 6.5 | 10.71 | 96 | Tonga | 13.6 | 30.0 | 150 | Ireland | 23.6 | 60.2 |
43 | Bhutan | 6.6 | 13.00 | 97 | Macedonia | 13.7 | 31.6 | 151 | Germany | 23.7 | 95.5 |
44 | Turkmenistan | 6.7 | 10.65 | 98 | Malaysia | 13.8 | 21.3 | 152 | Israel | 23.8 | 55.9 |
45 | Nepal | 6.9 | 11.60 | 99 | Ecuador | 13.9 | 18.6 | 153 | Netherlands | 23.9 | 80.7 |
46 | India | 7 | 41.00 | 100 | Jamaica | 14 | 34.9 | 154 | Japan | 24 | 176.7 |
47 | Iraq | 7.2 | 11.74 | 101 | Mauritius | 14.1 | 36.6 | 155 | Canada | 24 | 58.9 |
48 | Bangladesh | 7.6 | 10.31 | 102 | Dominica | 14.1 | 29.5 | 156 | Norway | 24.4 | 91.6 |
49 | North Korea | 7.7 | 24.12 | 103 | Oman | 14.2 | 10.2 | 157 | New Zealand | 24.6 | 57.9 |
50 | Philippines | 8.4 | 14.56 | 104 | Mexico | 14.3 | 30.4 | 158 | Switzerland | 24.9 | 99.1 |
51 | Guatemala | 8.5 | 18.87 | 105 | Serbia | 14.3 | 60.5 | 159 | Iceland | 25 | 72.7 |
52 | Indonesia | 8.6 | 17.62 | 106 | Iran | 14.4 | 21.2 | 160 | Australia | 25.7 | 62.4 |
53 | Bolivia | 8.7 | 20.80 | 107 | Armenia | 14.4 | 35.3 |
|
|
| |
54 | Vanuatu | 8.9 | 11.89 | 108 | Antigua and Barbuda | 14.6 | 24.3 |
Table 1: Intelligence parameter (ѰΔt, years) and mortality rate (MA, patients per 100 000)

The inter-seasonal monitoring of temperature (T oC) and specific rotation [α] (optical activity) of the dextran aqueous solution are shown in Figure 4. Arrows in Figure 4 marks the appearance of greenery on birches (a) and first snow (b). Estimation of the activation energy (ЕА), obtained from the Arrhenius approximation of the dependence of [α] on T for a dextran solution, gave a value of 0.38 kJ/mol, close to EA for physiological glucose solution - 0.33 kJ/mol [33]. A slight decrease in [α] dextran is observed with an abnormal increase in T in the first half of June 2019, in other periods the changes in [α] correlated with the seasonal dependence of the activity of plant metabolism.
Discussion
From data analysis of the Tables and approximations of the distribution by country of the global mortality rate from AD (MA) and intellectual potential (ΨΔt) (Figure 1, Figure 3), it follows that both demographic characteristics depend on the level of economic development of countries, and DA exponentially depends on ΨΔt. The ranking of countries on the rise ΨΔt led to the division of countries according to the level of intellectual and economic development into three groups, which in coordinates MA and ΨΔt in Figure 2d form three zones, highlighted by rectangles d1 (1-75), d2 (76-131) and d3 (132 -160), in brackets the numbers of countries in the Table. These zones correspond to the division of countries of the world according to economic criteria for weak (d1), medium (d2) and highly developed (d3). There are no sharp boundaries on the ΨΔt coordinate between the d1 and d2 countries of the groups, but they have significantly less intellectual potential and MA than those of the d3 countries. The average values of ΨΔt in d1, d2 and d3 groups grow in an arithmetic progression – 5.9; 14.4; 22.5 years, and MA in geometrical – 12.7; 36.5; 87.1 per 100,000 population.
Large values of MA in the d3 group can be associated with the civilizational, mental risk factor of AD, which is based on discrepancies between the professions of the post-industrial epoch and the level of mental development of workers. For some professions, a person may not have the necessary education and natural abilities, and the performance of others, on the contrary, suppresses his mentality. Both situations are fraught with chronic stress, which leads to the degradation of cognitive functions and harmful changes in the brain [34, 35]. Such changes can easily occur in the brain of a child, which is immature up to 10–12 years old [36], if scientifically unfounded technologies are used in the process of learning. For example, in Japan children are required to learn the left hemisphere syllable alphabet in combination with the right-hemispheric hieroglyphics before school and in primary school [37]. At the same time, inevitable distortions of the natural functional specialization of the brain hemispheres can subsequently provoke and strengthen the effects of the mental risk factor of AD, which ultimately leads to an increase in MA in Japan to a record value in the d3 group. For comparison, in China, teaching hieroglyphic literacy is not as accelerated as in Japan and, accordingly, MA in China is three times less than in Japan.
The high efficiency of the sapientation process of countries of the d3 group, located, as a rule, in the zone above 35-40o s. sh. in [11], they were associated with a low level of their insolation and average annual temperature, as well as with a high efficiency of the effect of CF during the night and early morning [12, 13, 14, 38, 39, 40]. In d1 countries, the relationship between these climatic and solar factors is reversed, which explains the low ΨΔt and MA values in these countries compared with the d3 group countries. The physical nature of CF is not known, a priori endows it with helicity and high penetrating power, which is not inherent in the corpuscular and electromagnetic radiation of the Sun. In principle, solar neutrinos possess such properties, however, its physical nature still remains an unsolved problem of the physics of elementary particles [12, 41]. It is believed [38] that CF activates the processes of self-organization in water-containing cooperative biosystems containing homogeneous chiral molecules or molecular complexes. For the intensity of the solar neutrino flux of the beryllium cycle, an annual rhythm was revealed [42], due to the difference in distance between the Sun and the Earth in winter and summer.
The increase in [α] value of dextran solution after March 22 (Figure 4) correlates with the process of spring awakening of plants and confirms the hypothesis of the participation of CF in the metabolism of living organisms. The effect of CF can be explained by numerous observations of the anomalous productivity of living organisms and, above all, living in the aquatic environment (Figure 5) [10, 40]. Correlations of diurnal changes [α] [14, 33] and blood concentrations of cortisol, sugar and melatonin (Figure 2) indicate an increase in CF activity at night. In addition to the time factor and violations of the night sleep mode, the activity of the CF will be influenced by geographical parameters (latitude, composition of the lithosphere, hydrosphere).
Cooperative effects in biosystems, and hence their sensitivity to CF, depend significantly on the T of the human body and brain (Figure 2). An important role in the cognitive functions of the brain is played by metabolic processes in the structures of the frontal-temporal lobes [36]. The kinetics of these processes depends on stationary T [43], the value of which is determined by the intensity of metabolic processes and the rate of removal of excess heat from the brain by venous blood and the bones of the skull. The latter process effectively proceeds through the bones of the inner walls of the paranasal sinuses of the skull, since they are ventilated with inhaled air having a T external environment.

Figure 5: Grayan's mussel growth (M) in the northwestern part of the Sea of Japan (1), W is the number of sunspots during the minimum years of its activity (W) from [10].
With its decrease at night and slowing down of metabolic processes in sleep, the brain's T decreases by ~1 °C [43]. It follows that the stationary T of the frontal lobes of the aborigines of countries of the d1 group may be higher by tenths of a degree [43] than among the aborigines of the countries of the d3 group. This difference in T will affect the metabolism of cognitive functions and the quantum effects in the fluidic media of the brain, ensuring its response to the effects of CF [12, 33, 43]. Normally and pathologies, brain fluid systems contain glucose, amino acids and amyloid protein precursors [44, 45, 46]. The effect of CF and a decrease in brain T during a night's sleep can trigger the association of glucose, amino acids [14, 46, 47] and the aggregation of precursor proteins into amyloid plaques and fibrils [46, 48]. Changes in the balance of right-left amino acids in the fluid systems of the brain [49] under the influence of CF and temperature can lead to mutations of the genes responsible for the metabolism of amyloid protein [4].
Conclusion
The demographic analysis of statistical data on mortality from AD showed that, in the post-industrial epoch, the inadequate realization of the human mentality in the process of professional activity becomes a significant epidemiological risk factor for AD. Herewith in developing countries a lack of competence prevails, and in highly developed countries, it may be supplemented by the suppression of the natural abilities of a person by work in the service sector. In both situations, the human psyche will be traumatized and irreversible deformations of the neurophysiology of cognitive functions will occur, which in old age can provoke the development of AD. This mechanism of action of the mental risk factor AD is confirmed by the exponential dependence of its distribution on the education index of countries The geography of the mortality rate from AD agrees well with the difference in the effectiveness of the chiral solar and temperature factors on the physiology of the cognitive abilities of the Aboriginal countries of the North and South.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
